Every new provider hears the same answer when they ask how long credentialing takes: “about 90 days.” Sometimes it’s 60. Sometimes it’s 120. Occasionally a payer surprises you and finishes in 30. The number is real, but it hides everything that actually matters about how the work gets done.
What most people calling it “90 days” don’t tell you is that those 90 days are not idle waiting time. There is a sequence (applications, primary source verification, committee reviews, contract execution, EFT setup) and each step depends on the one before it being done correctly. Skip a field on the CAQH profile and you don’t lose ten minutes; you lose three weeks while a payer’s queue rotates back to your file. Mismatch a taxonomy code between NPPES and PECOS and Medicare returns the application instead of approving it. This post focuses on the timeline specifically. For the full picture of how credentialing works end to end, see our complete guide to provider credentialing.
If you’re a new provider trying to plan your start date, a practice owner adding a clinician, or a billing manager trying to forecast cash flow, what you actually need is a week-by-week view of where the work happens, who’s doing it, and what tends to break.
That’s what this post is. No marketing fluff, no “streamlined process.” Just a real timeline.
What Credentialing Actually Is (and What It Isn’t)
Credentialing, enrollment, and contracting are three separate steps that get used interchangeably, and confusing them is where a lot of timeline planning goes wrong. Before walking through the weeks, it’s worth being precise about the words.
Credentialing is the verification process. A payer (or hospital, or network) confirms that you are who you say you are: your medical license is real and current, your education actually happened, your malpractice carrier exists, your work history checks out, and there are no disciplinary actions sitting against your name. This is done through primary source verification, which means the payer contacts the issuing institution directly rather than trusting a copy you provided.
Enrollment is what authorizes you to bill. Once a payer has credentialed you, they enroll you in their system, assigning you a provider ID, linking you to a tax ID, and configuring electronic claims. Without enrollment, claims bounce back even if your credentials are fully verified. Many practices learn this the hard way the first time they try to bill before EFT setup is complete.
Contracting is the agreement layer. It’s where reimbursement rates, fee schedules, and the legal terms of your participation get negotiated and signed. With government payers (Medicare, Medicaid) there’s no real negotiation; you take the published rates. With commercial payers, the contract phase is where the actual money gets decided, and it can run in parallel with credentialing or after it depending on the payer.
A provider who is “credentialed” but not “enrolled” or “contracted” cannot bill. All three have to land before the first clean claim goes out.
The Honest Timeline by Payer Type
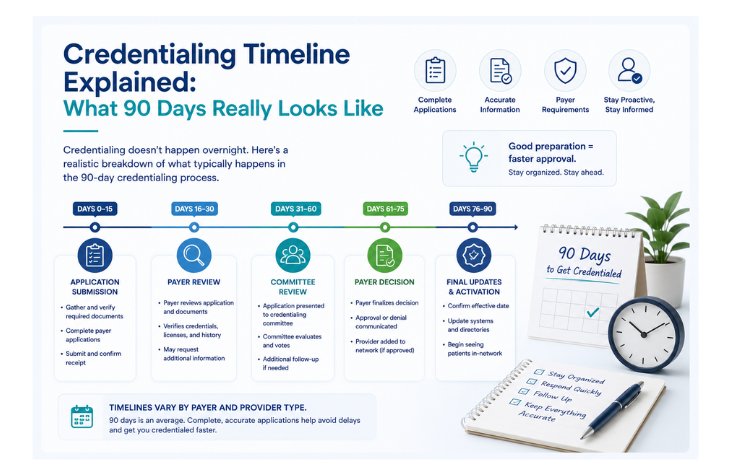
Most credentialing takes 90 to 120 days end to end, though it ranges from about 15 days for electronic Medicare submissions to 180 days for slow-state Medicaid. The “90 days” estimate exists because it’s a reasonable middle of the bell curve, but the spread is wide. Here’s what current data actually shows for 2026:
- Medicare via PECOS: Electronic submissions without a site visit typically process in about 15 days, with roughly 95% falling inside that window. When a site visit or development letter is involved, it stretches to 45 to 65 days. Paper applications add another 15 to 30 days on top of that.
- Medicaid: 45 to 180 days depending on the state. Florida and California tend to land in the 45 to 90 day range. Texas runs 60 to 120. New York is the slowest in the country, regularly hitting 90 to 180 days. Federal rules require states to process inside 45 to 90 days, but more than a dozen states routinely miss that standard.
- Commercial payers (BCBS, UnitedHealthcare, Aetna, Cigna, Humana): 60 to 120 days is the typical range, with some specialties and large network applications stretching to 180 days. Cigna’s published process runs 45 to 90.
- Hospital privileging: 60 to 120 days, often running parallel to commercial credentialing rather than after it.
- Telehealth-only credentialing through telehealth networks: 15 to 45 days, the fastest path in the industry.
Two patterns show up in the data that nobody likes to talk about. First, the average credentialing process is closer to 90-120 days than 60. Second, more than 80% of credentialing teams report that even basic enrollment tasks take more than 15 days to turn around, meaning small administrative steps consistently take longer than people plan for.
Week 1 to Week 2: The Foundation Phase
The single biggest predictor of how long credentialing takes is how clean your data is on day one. The first two weeks are not about waiting on payers. They’re about getting your house in order so the application is correct the first time.
The work happens in this order:
NPI verification. Every credentialed provider needs an active National Provider Identifier issued through NPPES. Group practices need both Type 1 (individual) and Type 2 (organizational) NPIs. Pull up your existing NPI in the registry and confirm that legal name, taxonomy code, and primary practice address all match what you’ll be putting on every payer application going forward. Mismatches between NPPES, PECOS, and CAQH are the single most common cause of downstream rejections.
Document collection. This is unglamorous but it’s where most delays start. You need:
- Current state medical license (not a temporary one, payers won’t accept those)
- DEA registration
- Board certification(s)
- Malpractice insurance certificate of insurance with current dates
- CV with no employment gaps left unexplained
- Diplomas from medical school, residency, fellowship
- Five years of work history with addresses and supervisor contacts
- Hospital affiliation documentation if applicable
- Government-issued ID and IRS Form W-9
If a date is wrong, a license is expired by even a day, or a gap in employment isn’t accounted for, the application will pause for a development letter, a payer’s way of asking for more information that adds two to four weeks per round.
CAQH ProView profile. If you don’t already have one, register at proview.caqh.org. CAQH assigns you a Provider ID, and roughly 75% of all credentialing transactions in the United States flow through this database. Roughly 80% of what Cigna, Aetna, BCBS, and most other commercial payers verify comes directly from your CAQH profile. The initial profile takes about two hours of focused work if your documents are organized; closer to a full day if they aren’t.
The CAQH profile must be 100% complete (no red asterisks remaining), all documents uploaded with valid expiration dates, and an attestation signed and dated. Then you have to authorize each target payer to access your data. A profile that’s complete but not authorized to a specific payer is invisible to that payer.
Realistic week 1 to 2 deliverables: NPI confirmed and aligned across systems, CAQH profile complete and attested, all supporting documents collected and uploaded, payer authorization list set.
If this phase drags into week 3, the entire timeline slides. Plan accordingly.
Week 3 to Week 4: Application Submission
With clean data in place, this is where you actually file applications. Two big strategic decisions sit here.
File Medicare first. This isn’t optional advice; it’s how the rest of the timeline works. Many commercial payers pull from PECOS to verify provider information, and some won’t finalize contracting until you have a Medicare PTAN (Provider Transaction Access Number). If you submit commercial applications before Medicare is approved, you may end up restarting parts of the commercial process when discrepancies surface.
Medicare enrollment runs through PECOS, the Provider Enrollment, Chain, and Ownership System. CMS rolled out PECOS 2.0 in 2025, which now pre-populates data across applications, requires multi-factor authentication via Identity & Access Management, and validates data more aggressively at submission. The upside is fewer downstream errors. The downside is that any inconsistency between PECOS, NPPES, and your supporting documents gets flagged immediately, and a “Returned” status stops the clock entirely until you correct and resubmit.
File commercial applications in parallel, not sequentially. Once Medicare is filed, the next step is to submit applications to every commercial payer you intend to participate with, simultaneously, not one at a time. Sequential filing turns a four-month process into a year. Each commercial payer pulls your CAQH data, runs their own verification, and reviews on their own clock. Filing in parallel means those clocks run in parallel.
For each commercial payer, this typically means:
- Submitting through CAQH ProView, OneHealthport, ProviderSource, or the payer’s portal
- Granting the payer electronic access to your CAQH data
- Filling out any payer-specific supplemental forms (behavioral health providers especially have these)
- Confirming receipt and getting an application reference number for tracking
By the end of week 4, you should have a tracking sheet with every payer, application date, reference number, expected decision window, and named contact at the payer.
Week 5 to Week 8: Primary Source Verification (The Black Box)
This is the part of the timeline where it feels like nothing is happening. It is also where the most time is actually spent.
Primary source verification is the payer (or its delegated credentialing verification organization) reaching out to:
- State medical boards to confirm license status and disciplinary history
- Medical schools and residency programs to verify education
- Previous employers to verify work history
- The National Practitioner Data Bank (NPDB) to query for malpractice and adverse actions
- DEA to confirm registration
- ABMS or specialty boards to confirm certification
- Sanction databases including OIG and SAM.gov
Each of those entities has its own response time. Medical boards in some states reply within days; others take six to eight weeks. Residency programs are notorious for slow responses, especially in summer when staff turn over. The NPDB query is fast (often same day), but if it returns a hit, it triggers an internal payer review that can add weeks.
There is very little you can do during this phase except respond fast when a payer’s credentialing analyst reaches out with a question. A development letter, a request for clarification or additional documentation, pauses the processing clock until you respond. A development letter that takes you a week to respond to costs you a week of timeline. One that takes three weeks costs you three.
The practical work in this phase:
- Check application status weekly through whatever portal each payer provides
- Respond to development letters within 48 hours (24 if possible)
- Keep your CAQH attestation current, since it expires every 120 days, and an expired attestation freezes commercial payer review even if your application is mid-flight
- Maintain a single point of contact at your practice for all payer outreach so nothing gets lost
By the end of week 8, Medicare should be approved or close to it, and most commercial payers should be in the credentialing committee review phase.
Week 9 to Week 12: Committee Review and Contracting
Most commercial payers run their credentialing decisions through a committee that meets on a fixed schedule, often monthly, sometimes every two weeks. This is why a file that completes verification on the wrong week can sit for an extra 30 days even though the work is done. There’s nothing to do about it except plan around it.
Once the committee approves, three things still have to happen:
Contract execution. The payer sends a participation agreement with the fee schedule attached. For commercial payers, this is where reimbursement rates get set. Contracts can be signed back the same day if you’re moving fast, or sit on someone’s desk for two weeks if nobody is pushing.
Directory listing. The payer adds you to their provider directory. Patients searching for in-network providers won’t see you until this is done, and the directory data has to match your CAQH and PECOS records exactly. A mismatched address here is the most common reason a credentialed provider can’t get patients to find them.
EFT and ERA setup. Electronic Funds Transfer and Electronic Remittance Advice configuration. This is the step that gets skipped most often, and the cost is direct. You can be fully credentialed, fully contracted, and still bouncing claims because EFT isn’t configured. It’s a separate enrollment workflow with each payer, often through a portal nobody told you about during credentialing.
By the end of week 12, the standard “90 days,” most commercial payers should be fully approved, contracts executed, and EFT configured. Medicare typically lands well before this. Medicaid varies wildly; in fast states, it’s done. In New York, it’s still pending and probably will be for another month or two.
What Actually Causes Delays
Most credentialing delays trace back to five recurring causes: incomplete CAQH profiles, data mismatches across systems, slow document responses, filing during peak seasons, and multi-state licensing complexity. The 90-day timeline assumes a clean process, and most processes are not clean. Across thousands of provider enrollments, the same patterns cause the overwhelming majority of delays.
Incomplete or expired CAQH profiles. If your CAQH profile is missing data, or attestation has lapsed past 120 days, every commercial payer’s review pauses. CAQH attestation is the single most common cause of delays across all payer types.
Data mismatches across systems. If your name on your medical license has a middle initial but your NPI doesn’t, or your practice address in PECOS is different from the one in CAQH, payers flag the application and request corrections. PECOS 2.0’s stricter validation has made these mismatches more visible than ever.
Slow document responses. When a payer asks for clarification, a missing date on a malpractice certificate, a gap in your work history, a hospital privilege confirmation, every day you wait to respond is a day added to the timeline.
Filing during peak seasons. January and July are notoriously slow because of new physician onboarding cycles. Holiday months see committee schedules thin out and applications back up. If you can avoid filing in late November or late June, do it.
Multi-state licensing. Telehealth providers credentialing in multiple states are running every step in parallel across multiple jurisdictions. Each state license requires separate verification, and Medicaid timelines compound across states. The Interstate Medical Licensure Compact (IMLC) helps, since physicians in 42 states plus DC and Guam can get expedited licenses in 14 to 21 days through the Compact, but it doesn’t cover all provider types.
Recredentialing lapses. This isn’t an initial-credentialing issue, but it’s worth flagging. Recredentialing is required every two to three years with most payers, and missing it terminates your network participation. Reinstatement is a full new credentialing cycle, which costs 90 to 180 days of revenue.
How to Move Faster
You can’t speed up primary source verification or committee schedules, but you can save meaningful time at the margins by starting early, filing electronically, keeping CAQH current, and assigning one owner. Some of the timeline is fixed; the rest is in your control.
Start early. Begin credentialing 120 days before the provider’s intended start date, not 60. The math is unforgiving: a provider who can’t bill is a provider whose salary you’re paying without revenue coming in. At an average physician revenue contribution of $2.4 million to $3.7 million per year (per Merritt Hawkins), every 30 days of credentialing delay translates to $200,000 to $300,000 of unrealized revenue.
File electronically wherever possible. PECOS electronic submissions process about 15 days faster than paper. Most commercial payers prefer electronic submissions through CAQH or a portal, and paper applications are routinely processed last.
Keep CAQH current quarterly, not annually. The 120-day attestation rule isn’t a suggestion. Build a calendar reminder for week 16 of every cycle, with a backup reminder for week 15. Multiple providers in a group means multiple attestation dates to track.
Designate a single owner. One person at your practice should own the application status of every provider with every payer. Distributed ownership creates dropped balls. Whether that’s an internal credentialing coordinator or an outsourced partner, the accountability has to be clear.
Track the small stuff. A spreadsheet with provider name, payer, application date, status, last contact date, and next action is enough. The fancy software is nice, but the basic discipline is what saves weeks.
If you want to see where your current credentialing data stands before you start, the free CredReady audit flags the mismatches and gaps most likely to slow a new application down.
What to Expect from a Credentialing Partner
If you’re outsourcing credentialing, what you’re paying for is not magic, since payers don’t move faster for outsourced applications. What you’re paying for is:
- Clean applications submitted right the first time, which is where most days are saved
- Active follow-up with payer contacts, so a development letter doesn’t sit unanswered for two weeks
- Tracking across providers and payers, so nothing falls through
- Knowledge of payer-specific quirks (which payer wants which form, who’s slow in Q4, which Medicaid state needs LiveScan fingerprinting)
- Recredentialing tracking, so a provider doesn’t get terminated three years later because nobody watched the calendar
A good partner will be able to tell you on any given Wednesday exactly where every application stands, who’s waiting on what, and when the next action is due. If you can’t get that answer in under five minutes, the partnership isn’t working.
A Realistic Plan for the Next 90 Days
If you’re a solo provider or a practice adding a clinician, here’s what a realistic plan looks like:
- Day 1 to 14: Document collection, CAQH setup, NPI alignment, target payer list finalized
- Day 15 to 30: Medicare PECOS submission, commercial applications filed in parallel
- Day 30 to 60: Primary source verification underway, weekly status checks, fast turnaround on any development letters
- Day 60 to 75: Medicare approved, commercial committee reviews scheduled
- Day 75 to 90: Contracts executed, EFT setup completed, directory listings confirmed
- Day 90+: Provider can bill across approved networks. Medicaid in slower states may still be pending.
The timeline assumes nothing goes sideways. Something usually does. Build in 30 days of buffer beyond the published estimate for every payer that matters to your revenue, and start the process before the provider’s first day rather than on it.
Frequently Asked Questions
Medical credentialing typically takes 90 to 120 days from start to finish, though the range is wide. Electronic Medicare submissions can process in about 15 days, commercial payers usually take 60 to 120 days, and Medicaid varies from 45 days in fast states to 180 days in slow ones like New York. The “90 days” estimate is a reasonable middle, but it assumes clean data and no development letters.
Most of the time is spent on primary source verification, where the payer independently confirms your license, education, work history, and sanctions with the issuing institutions. Each of those institutions responds on its own schedule, and some medical boards and residency programs take six to eight weeks. Committee review schedules, which often meet only monthly, add more time on top.
No. A provider who is credentialed but not yet enrolled and contracted cannot bill, and claims submitted before approval are typically denied. Some payers allow retroactive effective dates back to the application date, but many do not, so billing before approval risks uncollectible claims.
Credentialing is the verification of your qualifications. Enrollment is the payer adding you to their system and authorizing claims. Contracting is the agreement that sets your reimbursement rates. All three have to be complete before you can submit a clean claim, even though people often use the words interchangeably.
Start 120 days before the provider’s intended start date, file Medicare and commercial applications electronically and in parallel, keep the CAQH profile complete and attested, respond to any payer development letters within 48 hours, and assign one person to own the tracking. Most time savings come from submitting clean applications the first time rather than fixing rejections later.
Need Help With Credentialing?
Credentialing isn’t a one-time event. It’s an ongoing administrative function that determines how quickly new providers start generating revenue and how reliably existing providers stay enrolled. Practices that treat it as a side task tend to lose weeks of revenue every time they add a clinician or hit a recredentialing deadline.
MedBillingTech handles credentialing as a flat-fee service: $150 per application, with primary source documentation, application filing, follow-up, and status tracking included. We’ve handled credentialing across all 50 states for solo physicians, group practices, and telehealth providers, with sixteen-plus years of experience in payer enrollment.
Get a Free Credentialing Assessment →
Or call us at (512) 254-3133 to talk through your timeline.